Conceding that it has long been viewed as Republican-dominated, the industry's lobbying arm plans to spend tens of millions of dollars on an advertising blitz promoting Obama-style health coverage for every American. The first spot -- sponsored by the drug lobby, consumer and labor groups, and health providers -- will be unveiled today.Stop buying crap from dope heads...
Nothing less than H.R. 676, single payer universal health care, will solve our problems.
Everyone knows this is true.
----------------------------------
Single Payer Health Care Would Help Auto Industry
While I originally wrote this in January of 2007, concerning the cost of health care to consumers and service provided, it is equally applicable to the savings for the auto industry. And that is not my opinion, that is the opinion of the successful auto industry management. The ones that aren't asking for a bailout. At the time I wrote this in 2007, each vehicle assembled in the United States cost GM $1,525 for health care; those made in Canada cost GM $197. Probably more savings now since this was written nearly two years ago:
In U.S., it's pay more, get less - Universal Health Care
Why is this man smiling?In U.S., it's pay more, get less:
"A RELATIVE BARGAIN: George Mercieca, a worker at a GM assembly plant in Oshawa, Ontario, shows off his Canadian health care card. GM spends an average of $1,385 a year on medical bills for hourly workers in Canada. An American autoworker costs the company about $5,000, but studies show Americans are no healthier than their foreign counterparts."
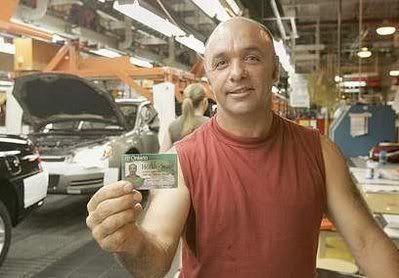
He is smiling because he has a great job with better medical benefits than most Americans could ever hope for under our failed health care for profit system. The kind of job that Connecticut , and the USA as a whole, can never hope to attract under our current system. If you do not believe me then ask yourself "what does the manufacturing industry have to say about this?"
While training issues are less of a problem here in Connecticut, because we have a decent educational system, health care is cited as a major issue for Toyota's decision to chose Ontario as the location of a new factory for their Rav-4s slated to open in 2008:
"The level of the workforce in general is so high that the training program you need for people, even for people who have not worked in a Toyota plant before, is minimal compared to what you have to go through in the southeastern United States," said Gerry Fedchun, president of the Automotive Parts Manufacturers' Association, whose members will see increased business with the new plant.
Acknowledging it was the "worst-kept secret" throughout Ontario's automotive industry, Toyota confirmed months of speculation Thursday by announcing plans to build a 1,300-worker factory in the southwestern Ontario city.
"Welcome to Woodstock - that's something I've been waiting a long time to say," Ray Tanguay, president of Toyota Motor Manufacturing Canada, told hundreds gathered at a high school gymnasium.
The plant will produce the RAV-4, dubbed by some as a "mini sport-utility vehicle" that Toyota currently makes only in Japan. It plans to build 100,000 vehicles annually.
The factory will cost $800 million to build, with the federal and provincial governments kicking in $125 million of that to help cover research, training and infrastructure costs.
Several U.S. states were reportedly prepared to offer more than double that amount of subsidy. But Fedchun said much of that extra money would have been eaten away by higher training costs than are necessary for the Woodstock project.
He said Nissan and Honda have encountered difficulties getting new plants up to full production in recent years in Mississippi and Alabama due to an untrained - and often illiterate - workforce. In Alabama, trainers had to use "pictorials" to teach some illiterate workers how to use high-tech plant equipment.
"The educational level and the skill level of the people down there is so much lower than it is in Ontario," Fedchun said.
In addition to lower training costs, Canadian workers are also $4 to $5 cheaper to employ partly thanks to the taxpayer-funded health-care system in Canada, said federal Industry Minister David Emmerson.
"Most people don't think of our health-care system as being a competitive advantage," he said.
It is clearly an advantage for any company that wants to open up a business in any industry... A 4 to 5 dollar per hour advantage. An advantage so great that any state that passes true-single-payer Universal Health care first will be positioned to become a mecca for any company considering opening any kind of business.
We already have an educational advantage over the most of the USA, having a highly rated school system and a high rate of college graduates. Why the hold up on giving these businesses the real money savings that Universal Health Care would provide and the other best reason to set up shop in Connecticut?
Because of lobbying from the insurance and pharmaceutical industries. We need to take them out of the loop in the decision making process for this issue since we know they will fight it tooth-and-nail. We need to look at what is best for the people of Connecticut and for all industries, not just those two lobbying behemoths.
And just how much more is health care costing us?
Medical bills soar
Divide the nation's medical bill evenly across the population, and each of us paid $6,102 in 2004, according to the Organization for Economic Cooperation and Development. That's 50 percent more than the residents of the country with the next-highest health care bill, Switzerland ($4,077), and more than double the average for industrialized nations ($2,546).
...snip...
Those countries provide health care for all their residents for less money than the United State spends while it leaves an estimated 46 million without insurance.
That's contradicted by studies conducted by Gerard Anderson, director of the Center for Hospital Finance and Management at Johns Hopkins School of Public Health. "We have about the same number of MRIs and CT scanners as Canada, the U.K. and France, and far fewer than Japan," Anderson said. "We have the same number of doctors, doctor visits, hospitals and inpatient days at hospitals.
"The difference is we pay two to 2 1/2 times more for virtually identical services."
The average U.S. physician earned $180,000 in 2004, Anderson said; in Canada, it was $100,000 (in U.S. dollars).
Even after adjusting for the higher income of U.S. residents, Americans pay on average $2,000 more per year for health care than the residents of the next-highest paying country, Anderson said.
One out of every seven dollars spent today in the United States goes for health care -- a record 15.3 percent of the gross domestic product in 2004, the latest year for which statistics are available. By comparison, Canada spends 9.9 percent of its GDP; Japan spends 8.0 percent.
By 2015, one out of every five dollars spent in the United States will go for health care, according to projections by the Centers for Medicare and Medicaid Services. If those projections hold, the average American's share for medical needs alone will be a staggering $12,320.
For all that money, you would expect Americans to be healthier than their foreign friends. The opposite is true.
Whoa! They are healthier than us, and they pay less? And it is not just a monetary cost:
If you're born in the United States, chances are that you'll die younger than people born in other industrialized nations. The United States has the lowest life expectancy of 14 nations measured by the World Health Organization. U.S. life expectancy in 2001 was 77.1; Canada, 79.7; Italy, 79.8; Japan, 81.5
The infant mortality rate is higher in the United States than in other industrialized nations. In 2003, seven infants died for every 1,000 live births in the United States -- the worst rate of 19 countries measured by the Organization for Economic Cooperation and Development.
I am thinking that anyone that is really PRO-LIFE, and not just talking about it for political reasons, would have to be shocked by those infant mortality rates. Why aren't they screaming about this issue? If they are really honest about being pro-life than they should be our allies on true Universal Heath Care.
As for manufacturers, just how much profit margin can health care open up for them?
Those vehicles, often parked on the same dealer lot as identical vehicles produced in U.S. plants, have one notable difference: Each vehicle assembled in the United States cost GM $1,525 for health care; those made in Canada cost GM $197.
The higher salaries of Canadian autoworkers offset much of the health care savings for the company, said Jim Cameron, labor relations director for GM Canada. But at the cash-strapped automaker, such a huge health care cost differential is hard to ignore. The difference is primarily a result of Canada's national health care system, in which most medical bills are paid by the government. Most countries have similar systems.
WHAT THE FUCK!!! The GM employees get higher wages up there too? And GM still racks up more profits from production up north in Canada then they can down here? How much more of this are you Nutmeggers willing to take?
Can you imagine the shockwave across the nation if a car manufacturer or some other large industry chose to locate in Connecticut over other states or countries... And it could happen.
Do you want to continue to pay more just to get less? Less healthy workers, less money, less jobs, less profit for industry as a whole.
Why not get more? More people that actually have coverage? More healthy workers that are more productive? More savings in health care for us and for industry? More manufacturers picking Connecticut as their destination of choice? More smiles on Nutmeggers' faces.
Universal Health Care is the answer to everyone getting more.
_______________
It might be the answer to save US industry.
There is an off the shelf answer sitting there getting dusty. Ask Rep. John Conyers, Rep. Dennis Kucinich and the other cosigners about H.R. 676. It would be a huge step towards helping every industry in this nation become competitive.
If you need to know about a health care plan that can fix many of the problems with our privatized ripoff:
The United States National Health Insurance Act
"Expanded & Improved Medicare For All"
*introduced by Reps. John Conyers, Dennis Kucinich, Jim McDermott and Donna Christensen
If you live in CT-05 you may want to know that Rep. Chris Murphy has yet to sign up as a co-sponsor to this bill. Ya think it is time to remind him how important H.R. 676 is to all Americans?
Rep. Chris Murphy's contact info
Chris Murphy
(202) 225-4476,
1 Grove Street, New Britain CT 06053
If you live elsewhere, you might want to consider contacting your own Congress critters, as well.
_______________
(here are some reactions from a recent re-posting of this diary from around the internet added to it below.)
Some more actions we can take to bring this change, via Bruce Dixon at the Black Agenda Report:
What We Can Do to Protect US Jobs, Accomplish Universal Health Care, and Hold the New President Accountable.
- Get the information about single payer health care and spread what the corporate media won't.
Be a frequent visitor at the web site of Physicians for a National Health Care Plan, http://pnhp.org. There you will find research material, talking points, frequently asked questions and answers, press releases and new information every day, enough to answer anybody's questions on single payer, and to provide answers to all the lies and propaganda spread by the insurance companies. This is the stuff to write about, to blog about, to send and forward to everyone on your email list.
- Email, call and visit your member of Congress about single payer health care and saving US jobs.
Whether they already support HR 676 or not, remind your elected representative that US industries cannot compete with those in societies which offer free health care. Demand that single payer health care ought to be part of any legislative deal to save US auto companies.
Phone calls and emails are good. Letters and faxees are better. But group visits of five or more people to district offices are the most potent weapons of persuasion. Organize one. Nearly all members of congress have open hours during which constituents can make an appointment with or drop in on the Great Man or Woman to discuss issues of importance. If you video any of these visits, we will be happy to post them here, and in some cases if you organize the visit, we can arrange to shoot the video. Email us for details.
- Call a public meeting or teach-in at your school or neighborhood to talk about single payer health care.
Pnhp.org and others can help you arrange authoritative and knowledgeable speakers. Video that too so others not present at the event can see it.
This is not the time to lay back, to wait and see what the new administration does or wants to do. Every day we wait before organizing to inform each other and publicly pressure the new president and his party to keep their promises is a day that the parasitic private health insurers enjoy unrestricted and unfettered access to the new administration behind the scenes. Elite pressure occurs behind the scenes. Pressure in the public interest is --- well --- public.
This won't be easy. Nearly every Democratic president since Harry Truman has aimed at some kind of solution to the health care mess. Producing an aroused public makes it easier for the new administration and its party to do the right thing. But if we don't get loud about the link between saving jobs and delivering health care early in an Obama administration, a precious opportunity will be lost that we may never see again.
And... Just to be clear on what the auto industry really thinks about single payer universal health care, from tiggers thotful spot at TPM:
Yes, (The best way to 'rescue' General Motors is single payer health care) great minds think alike.
This is from a letter that the Big Three executives SENT to the Canadian govt:
The public health care system significantly reduces total labour costs for automobile manufacturing firms, compared to the cost of equivalent private insurance services purchased by U.S.-based automakers; these health insurance savings can amount to several dollars per hour of labour worked. Publicly funded health care thus accounts for a significant portion of Canada's overall labour cost advantage in auto assembly, versus the U.S., which in turn has been a significant factor in maintaining and attracting new auto investment to Canada...
For both employers and workers in the auto industry, it is vitally important that the publicly funded health care system be preserved and renewed, on the existing principles of universality, accessibility, portability, comprehensiveness, and public administration...
From Ozzie, a couple of videos discussing single payer health care:
Nick Skala, formerly of PNHP and co-founder of Health Care for All Illinois details quite a bit.
Part 2 here.
From Imavehmontah on savings with single payer universal health care:
Single payer healthcare means replacing the present patchwork quilt of payment mechanisms for the cost of health care with a single point source payer. That single payer is responsible for defining the benefits package that is covered, actuarial predictions of what the cost would be for those services, collecting the money required to cover those costs, and disbursement of the money. The single payer obviously has a great amount of power and responsibility for health care. There may or may not be the addition of other payers for services that are outside of the benefits package chosen by the single payer. Some single payer systems have also allowed people to "opt-out" of being covered by a single payer system and go it alone, with or without the help of other insurance companies or plans.
Why is single payer advantageous? There are a number of ways that single payer plans (can potentially) improve care and reduce costs:
When all people are in a large common pool, the single payer has enormous leverage to negotiate prices.
When all people are in a common pool, the single payer can prospectively look at the relative values provided by different modes of treatment and decide which modalities are most cost effective for the populace at large.
The single payer can preferentially fund and reward preventive care (which may even include preventions typically not thought of as "health care" like smoking cessation), which frees up resources that may otherwise be wasted.
The single payer can reduce greatly the amount of resources required to get reimbursement for service provided, freeing those resources to be used for other health care services.
The single payer can reduce geographic maldistribution of health care resources.
The single payer has no fear that money invested in services that keep people healthy will become a reward for someone else down the line as people change health care plans.
Being involved in a single payer system raised the awareness and accountability of all of participants in the system. It quickly becomes clear that it is in your interest to make sure that your neighbors take advantage of preventive services and behaviors because everybody wins.
A single payer plan can (if properly designed) be more responsive to local needs and variations, and more locally accountable.
A single payer system can improve the use of health care technology for information use that will give us a clearer picture of how to allocate resources for the best return on investment.
A single payer system can greatly reduce the percentage of the total GNP that health care consumes, benefitting all industry.
Now, there are going to be a lot of anecdotal replies to this about this description. I admit that not all single payer implementations realize these potentials. But nonetheless these are the possible benefits in a well designed system.
neroden on systems eliminated by single payer universal health care:
I'll count Medicare (parts A and B) as continuing to exist, because they would likely form the basis of the single payer system. If the single-payer system was "built fresh" they would go away too.
(1) All private insurance companies, including all HMOs and PPOs. There might be a small number left to provide "supplemental" insurance.
(2) Medicaid. Subsumed by single-payer.
(3) S-CHIP. Subsumed by single-payer.
(4) Medicare [Dis]Advantage. This is private companies.
(5) Medicare Part D. Elimination of private companies.
(6) Health care compensation from auto insurance. (Compensation for lost wages and "quality of life" would continue, but would be much simpler to adjudicate; premiums would drop).
(7) Health care compensation for 'worker's comp'. (Compensation for lost wages and "quality of life" would continue, but would be much simpler to adjudicate; premiums would drop.)
(8) "preferred providers", doctors accepting some insurances and not others, and all similar doctors' office paperwork. Every doctor would either be "in the national system" or not, and very few would not.
(9) State and local health insurance systems for their employees. Subsumed by single-payer.
(10) Self-funded insurance schemes from corporations (like GM) and universities (like Cornell). Subsumed by single-payer.
(11) Special "flu clinics" and other such schemes for getting basic preventative medicine to everyone. Everyone would have a regular doctor in the system and that doctor would offer preventative medicine for free.
(12) Health care aspect of disability insurance for business. (Compensation for lost wages would continue, but would be much simpler to adjudicate; premiums would drop.)
(13) Federal government employees insurance system. Subsumed by single-payer.
(14) Charity care budgets at emergency rooms. Subsumed by single-payer.
It would instantly save many corporations, hospitals, and individuals from bankruptcy.
Current estimates are that the tax increase needed would be very small. The administrative savings from combining Medicare, Medicaid, S-CHIP, and the Government Employees insurance program is substantial; the savings from pricing power are large; and the government already covers all the people with the highest health care costs (children, the elderly, the poor, and the military), so adding all the "cheap" people costs a lot less proportionally. Estimates are that the government already pays 7/8 of all health care spending in the country, so that gives you a good sense of the necessary increase.
People relatively well-to-do would presumably see their taxes go up slightly, as would well-to-do businesses. However, almost anyone who is actually paying for their insurance would end up saving money. Only people who are uninsured and healthy (who benefit by getting coverage), or who have their insurance entirely paid for by employers (which is very rare these days) would have a net increase in costs.
What it would require is firing a lot of people -- the people working for the health insurance companies, or working in other offices to deal with the health insurance companies. That's where the out-of-pocket savings for most Americans would come from: the fired paper-pushers. That is the actual downside: elimination of jobs, but since they're wasteful make-work, or even make-trouble, jobs, I think it's worth it. We could come up with a job placement program for them.
While it would eliminate insurance company jobs that PRODUCE NOTHING (except for the leeching effect off of our paychecks) these jobs would be replaced by more productive jobs in the health care industry. More Doctors, Nurses, technicians and other supporting jobs for hospitals, clinics and industries that produce health care products.
Jobs that would be more beneficial to individuals, industry and to society as a whole.